How is the procedure performed?
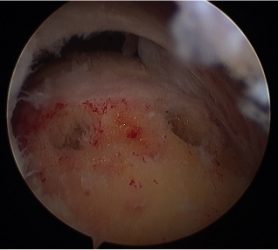
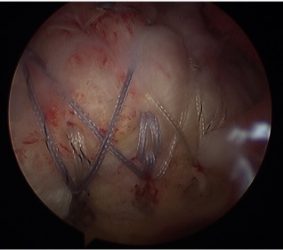
The procedure is performed under a combination of general and regional anaesthesia. Most rotator cuff repairs are performed arthroscopically but repair of some large tears may be carried out through an “open” procedure. The inside of the joint and subacromial bursa are examined. A small amount of bone is removed from the undersurface of the acromion. The bone where the tendon normally attaches is freshened to promote bleeding and facilitate healing. The tendon is then fixed back to bone with suture anchors.
Additional procedures
Other procedures such as an acromioclavicular joint excision, biceps tenotomy or tenodesis, labral repair or capsular release may be performed, if indicated, at the same time. If the tear is very big or if the tendon quality is poor, the repair may be reinforced with a “patch” of donor tissue. If the tear is found to be irreparable, a superior capsular reconstruction may be performed.
Alternatives
The alternatives to surgical repair of the torn rotator cuff are to do nothing or continue with physiotherapy and exercises.
Benefits
The main benefit of the procedure is to relieve pain and improve the function of the joint and ability to use the arm. More than 85% of patients achieve benefit from surgery.
Risks
The overall risk of complications is approximately 10%.
Pain - The shoulder may be painful for some weeks after surgery. Pain is managed with medication.
Swelling – When performed arthroscopically, the joint is distended with saline and this may lead to the shoulder remaining swollen for a day or two after surgery.
Bleeding – A small amount of bleeding from the arthroscopy portal sites or skin wound is not unusual and will usually settle after a day or two.
Stiffness – This occurs in approximately 8% of patients. Prevention is the key and it is essential to follow the instructions provided, perform daily passive stretching to maintain the range of movements. If stiffness persists over a number of months, then occasionally further treatment may be necessary.
Irreparability – Some tears may not be reparable owing to the tendons being fragile or inelastic or the tear being massive. In such instances a partial repair may be performed with a satisfactory outcome. In specific instances an alternative procedure such as augmentation with an allograft patch or a superior capsular reconstruction may be performed.
Failure of healing – Occasionally the tendon may fail to heal. This is more likely if the tear is large, the tendon quality is poor or if the tendon is not protected in the early phase after surgery. Smoking impairs healing and should be stopped before surgery and avoided afterwards.
Hardware failure – Suture anchors may rarely work loose from the bone. This will often require further surgery to remove the loose anchors.
Infection – Infection is a possibility but is rare after arthroscopic surgery.
Nerve injury, Complex regional pain syndrome, Venous thromboembolism – These are possible but rare.
Aftercare
- Following the procedure the arthroscopy portal sites /skin incision will be closed with buried sutures and tape and covered with shower-proof dressings. These dressings should be left undisturbed as far as possible for 5-7 days. If the dressings are removed for any reason they should be replaced with similar dressings or waterproof plasters. The dressings may be removed one week after surgery as the skin should be healed by then.
- The shoulder may also be covered with an absorbent pad (or a nappy). This will usually be removed the day after surgery.
- Your arm will be placed in a sling after surgery. Prior to discharge from hospital a physiotherapist will provide instructions about looking after the shoulder and managing life with a sling.
- You will be advised on how to protect the repair and intermittently perform limited passive movements of the shoulder only for the first 6 weeks. After 6 weeks you will be allowed to move the shoulder actively and may resume driving. Strengthening exercises are started after 12 weeks or when satisfactory movements and control have been regained. Outpatient physiotherapy will be arranged and may be continued for 6-9 months after surgery.
- You will be unable to drive for at least 6 to 8 weeks.
- For detailed instructions on rehabilitation click here.
Follow-up
An appointment will be arranged for you at 2-4 weeks after the procedure. Follow-up is required for at least 6-12 months after surgery or until a satisfactory recovery is achieved.