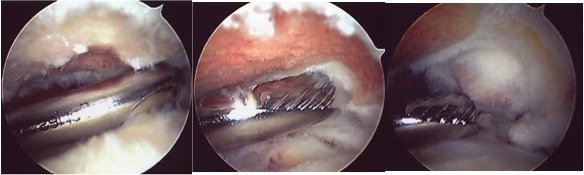
How is the procedure performed?
The procedure is performed under a combination of general and regional anaesthesia. An arthroscope is inserted into the joint after distending it with saline. The inside of the joint and subacromial bursa are examined. The undersurface of the acromion is exposed with the aid of a radiofrequency probe and a small amount of bone is removed with the aid of an arthroscopic shaver (motorised burr).
Alternatives
The alternatives to surgery are to do nothing (let nature takes its course) or continue with physiotherapy and exercises.
Benefits
The main benefit of the procedure is to relieve pain associated with movements. This is will in turn allow an improvement in the function of the joint and ability to use the arm. More than 90% of patients achieve benefit from surgery.
Risks
Swelling – During the procedure, the joint is distended with saline and this may lead to the shoulder remaining swollen for a day or two after surgery.
Bleeding – A small amount of bleeding from the arthroscopy portal sites is not unusual and will usually settle after a day or two.
Stiffness – This may occasionally occur after any form of shoulder surgery. Prevention is the key and it is essential to follow the instructions provided, perform daily stretching and exercises at home to maintain the range of movements. If stiffness cannot be overcome with physiotherapy over a number of weeks, then occasionally further treatment may be necessary.
Dissatisfaction - A small proportion of patients may experience persistent symptoms despite surrgery. Whilst this is uncommon, it may indicate that the pain is from a different source.
Infection – Infection is a possibility but rare after arthroscopic surgery.
Nerve injury – Injury to the nerves around the shoulder is possible but extremely rare.
Aftercare
Following the procedure the arthroscopy portal sites (skin incisions) will be closed with tape or sutures and covered with shower-proof dressings. These dressings should be left undisturbed as far as possible for 5-7 days. If the dressings are removed for any reason they should be replaced with similar dressings or waterproof plasters. The shoulder may also be covered with an absorbent pad (or a nappy). This will usually be removed the day after surgery. A sling will be provided to support the arm, but may be removed as tolerated to move the arm and is usually discarded after 2-3 days. A physiotherapist will provide instructions about mobilising the shoulder prior to discharge from hospital. You may resume driving within 3-4 days. Outpatient physiotherapy may occasionally be recommended but is not always necessary.
Resuming work, driving and activities
You may resume driving within 4-5 days or when you have regained sufficient movements and control of the arm. Office duties may be resumed within 5-7 days. Manual work should be avoided for at least 6 weeks. Non-contact sports may be resumed at 6 weeks.
Follow-up
An appointment will be arranged for you in the outpatient clinic at 2-4 weeks after the procedure. Follow-up is required for at least 3-6 months after surgery or until a satisfactory recovery is achieved.