How is bursitis of the elbow diagnosed?
The condition usually presents with a lump on the back of the elbow, which is often painless. Some patients may experience discomfort or occasionally a burning sensation on the back of the elbow, particularly when leaning on the elbow. In case of an infection, the swelling may be associated with fever.
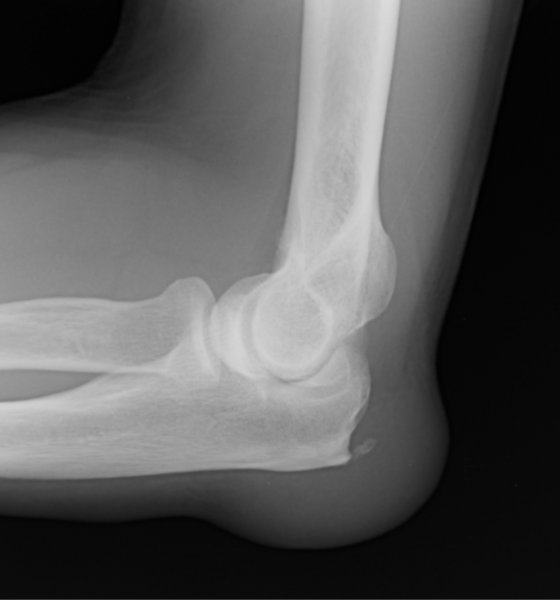
Examination of the joint shows a soft lump on the back of the elbow. There may be redness and warmth if there is an underlying infection. An X-ray may be performed to look for bone spurs and to assess the joint surfaces. Blood tests may be arranged to exclude gout.
How is bursitis of the elbow treated?
If the lump is painless and not causing symptoms then no treatment may be necessary.
Noninfective bursitis
Aspiration: If the lump is causing discomfort, the fluid may be drawn off with a needle using an aseptic technique to reduce the size of the lump. A sample of fluid is sent to the pathology laboratory for microscopic examination. Injection of steroid may reduce the risk of recurrence but carries additional risk. The fluid may reaccumulate after aspiration.
Surgery: Surgical treatment may be considered in some patients, in whom symptoms are troublesome or interfere with sports or work, or if the lump is large and unsightly. The elbow is explored through an incision on the back of the elbow, the fluid is drained and the lining of the sac is removed to prevent recurrence. In selected cases this may be accomplished with arthroscopic surgery. A new bursa will reform over a period of time.
Infective bursitis
Aspiration: Drawing the fluid off with a needle and syringe will reduce the size of the lump and the associated discomfort and provides a sample of fluid for microbiological examination to help identify the causative organism.
Antibiotics: When treated early an infective bursitis may respond to treatment with a course of appropriate antibiotics. Ideally, antibiotics should not be started until a sample of fluid has been aspirated for microscopic examination
Surgery: If the swelling is large or has recurred despite treatment with antibiotics, then surgery should be considered to drain the infected fluid and remove the lining of the bursa in its entirety.